


Beyond Branding, Make it Personal
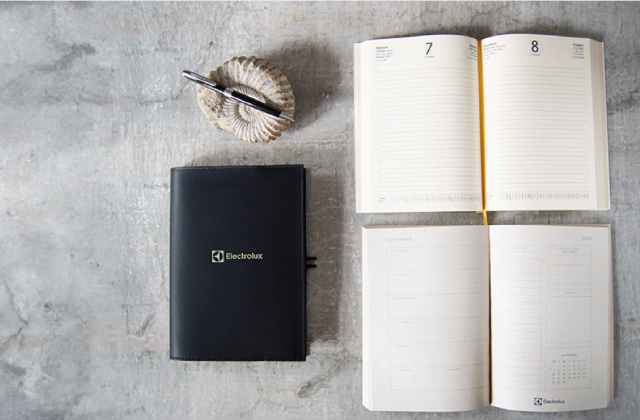
When we established the branding segment of our business we saw a gap in the market for high quality branded personalised products at reasonable trade level prices. The market seemed to be split in two, high-end luxury goods or soulless plastic usb sticks. At Creatico we aim to bridge that gap.
Our corporate tiered pricing scheme is openly published and our fees totally transparent. Hand debossed logo branding is always included in the price.


Brands we have worked with:






Our Brands:








Things we are Passionate About:

Ethical & Handmade
We are proud to have worked closely with the same supply partners for over 20 years. This level of synergy and shared success is integral to our identity.
LEARN
Crisp Personalisation
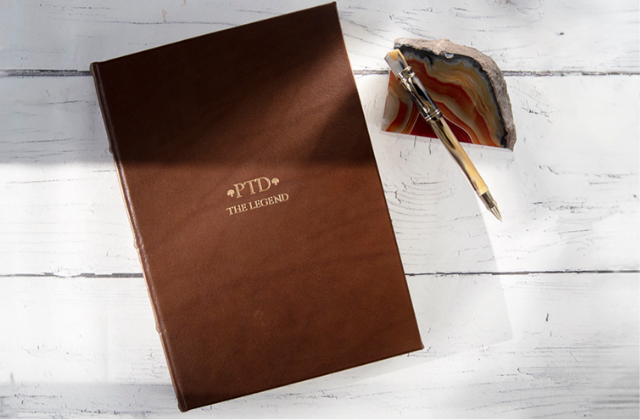
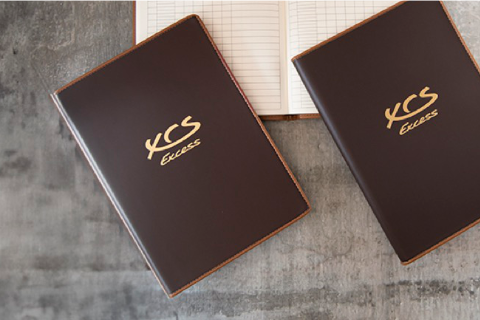
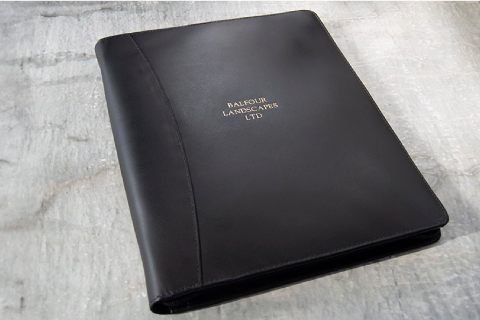
All personalisation is in house, each monogram or logo is pressed by hand, using quality brass type providing a clear and most precise impression into the leather.
LEARN
Attention to Detail
The little things matter. We strive to provide a seamless service and a long lasting impression for you and your clients. We would like to have your order, but what we truly want is your business.
LEARN

Country
Request Free Visual & Quote
Preciso A5 Journal
Newsletter
we just need a few more details